
Measuring What Matters: How Measurement-Based Care Is Advancing Outcomes for Children and Youth in New England
By Simon Weisz, President & Co-Founder, Greenspace Health
"MBC offers the ability to, if in doubt, zoom out. It helps the teen see their own data rather than the clinician or someone else saying, 'I think you're doing better.' For teens particularly, with their autonomy needs, the fact that they're able to look at their own ratings is significant and helps the clinical process."
- Dr. David Fitzgerald, Assistant Professor of Psychiatry at UConn Health

Behavioral health providers across New England are facing a sharper accountability moment than perhaps any in recent memory. Federal funding cuts, Medicaid uncertainty, and rising expectations from payers and accreditors mean that Measurement-Based Care is becoming essential infrastructure, particularly in child and youth behavioral health where the stakes are highest.
What Is Measurement-Based Care, and Why Does It Matter for Children and Youth?
Measurement-Based Care (MBC) is the routine collection of validated, patient-reported outcome measures (PROMs) to track symptoms and progress over time, with the resulting data used to inform clinical decision-making. In practice, it means a young person completing a standardized assessment at each visit, their clinician reviewing the results together with them, and that data shaping the direction of care.
The research case is well established. Studies consistently show that MBC helps clinicians identify deterioration earlier, adjust treatment more effectively, and improve outcomes. In child and youth settings, this is particularly important as young people are less likely to spontaneously report worsening symptoms, and developmental factors can mask clinical signals that a validated tool would surface.
"MBC offers the ability to, if in doubt, zoom out. It helps the teen see their own data rather than the clinician or someone else saying, 'I think you're doing better.' For teens particularly, with their autonomy needs, the fact that they're able to look at their own ratings is significant and helps the clinical process."- Dr. David Fitzgerald, Assistant Professor of Psychiatry at UConn Health
The New England Context: Funding Pressure Is Accelerating Adoption
New England’s children’s behavioral health system is at an inflection point. NECBHN has identified the convergence of Medicaid uncertainty and the expiration of pandemic-era school funding as a potential “perfect storm” for behavioral health reimbursement today.
At the same time, quality expectations are rising. Emergency department volumes have declined as access has improved, shifting the policy conversation from capacity to outcomes. Understanding what care works, and for whom, is becoming a competitive and contractual necessity. As the system continues to evolve, increased use of MBC is going to be key to across accreditation, contracting, and grant environments simultaneously:
Accreditation: CARF and The Joint Commission increasingly expect structured outcomes measurement within behavioral health services.
Grant reporting: Federal funders including SAMHSA increasingly expect applicants and recipients to demonstrate outcomes using validated measures.
Value-based contracting: As Medicaid managed care and value-based payment models expand, payers are looking for partners who can demonstrate patient-level outcomes. MBC data provides exactly the evidence at the client, program, and population level needed to unlock meaningful ROI for behavioral health organizations.
"MBC made it much easier to go back to the agencies that were supporting this and say, look, 70% of our kids showed reliable improvement on this measure. And so that made it a lot easier to write the year-end summaries and to get funded for subsequent years." - Dr. David Fitzgerald, Assistant Professor of Psychiatry at UConn Health
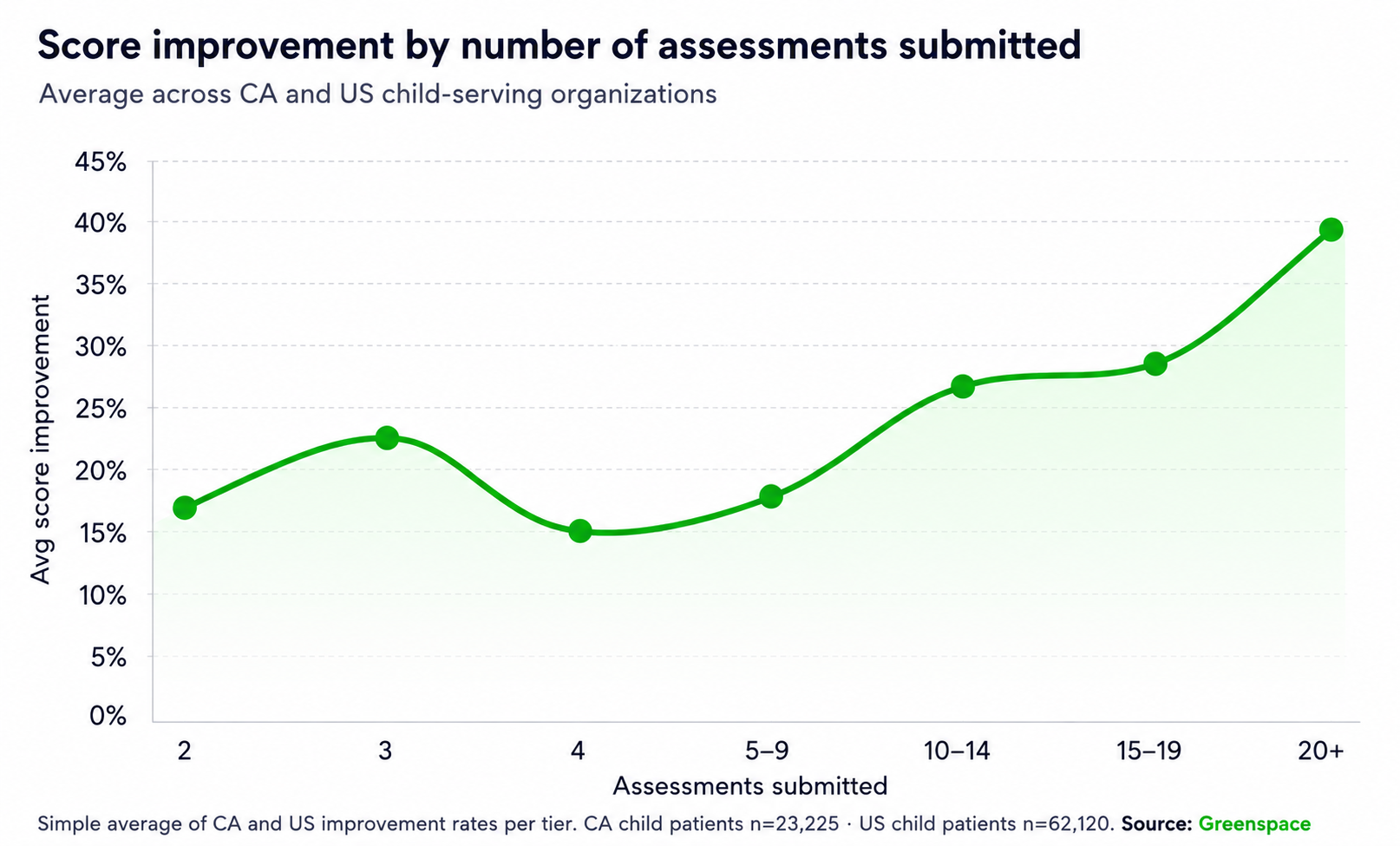
Across the child and youth organizations using the Greenspace MBC platform, the data tells a consistent story. On average, children and youth show a 37% score improvement over the course of treatment, with therapeutic alliance scores holding strong at 85%. That improvement isn't static; child patients who complete 20 or more assessments show nearly 2.5 times the clinical improvement of those who complete just two, underscoring that sustained engagement with measurement deepens outcomes over time.
Roughly one in three youth clients using Greenspace meet the threshold for reliable improvement and nearly 40% reliably recover. These patterns are consistent with what the broader research literature predicts, and they provide the kind of documented, program-level evidence that funders and accreditors are increasingly asking for.
Getting It Right: Implementation in Child and Youth Settings
The most common concern we hear from providers is practical: how does MBC work with children, and how do we build it into existing workflows without adding burden? A few principles that distinguish successful implementations:
Choose developmentally appropriate tools. Select validated, age-appropriate measures that match your population and service scope.
Embed MBC as a clinical tool, not a compliance metric. Frame it from the outset as a support for clinical decision-making and treatment formulation.
Make data visible and meaningful for young people. Share graphs, review trends together, and invite young people to interpret their scores.
Use aggregate data at the program level. Aggregate dashboards help identify which groups or presenting problems are associated with slower progress.
Build it into supervision. Reviewing client scores in supervision normalizes MBC, strengthens clinical skill over time, and creates a natural mechanism for catching cases that may need a different approach.
Integrate. Integrate MBC into existing workflows and EHR systems where possible to reduce friction.
Build reporting infrastructure. The organizations that get the most from MBC are those that prioritize client needs, while keeping funders, accreditors, or payers in mind from the beginning, so they can build the data infrastructure to answer those questions from day one.
The Bottom Line
MBC is the best we can do for clients and for long-term organizational sustainability. Organizations must build the infrastructure and culture that empowers providers to do it in a way that genuinely improves care for children and youth, builds the data foundation for financial sustainability, and doesn’t overwhelm already-stretched clinical teams.
The good news is that the evidence is clear, the technology and infrastructure are available, and the providers who have implemented MBC thoughtfully are demonstrating that it works, both clinically and operationally.
———————————————————————————————————————————————————————
Interested in contributing to our blog? We welcome perspectives from researchers, clinicians, policymakers, advocates, and community members working to advance children's behavioral health. If you'd like to contribute to a future blog, please reach out to us at info@necbhn.org.
